Ulnar neuritis
Cubital tunnel syndrome
Ulnar neuritis, also known as cubital tunnel syndrome, is a condition where the ulnar nerve becomes compressed or irritated. The ulnar nerve travels down the arm all the way to the pinky. The section of nerve that travels through the elbow is the most common section that is compressed. Ulnar Neuritis can result in other conditions such as muscle wasting (muscles begin to waste away) if not treated quickly enough. There are both surgical and nonsurgical treatments available, and both lead to good results.
Anatomy
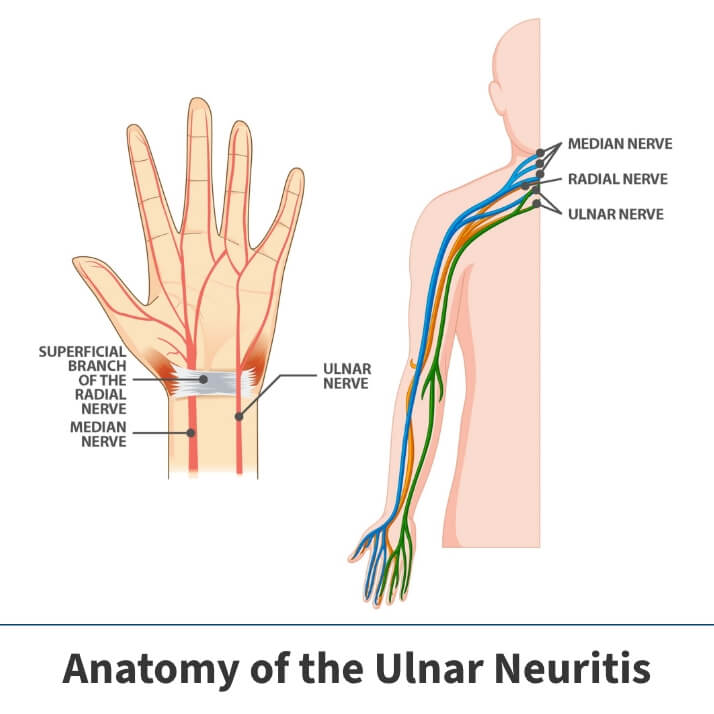
The ulnar nerve gives feeling to the little finger and half of the ring finger while also controlling most of the small muscles in the hand, as well as some bigger muscles in the forearm. It travels through a tunnel of tissue called the cubital tunnel, which runs under a bump of bone at the inside of the elbow known as the medial epicondyle. This area in the elbow is commonly known as the “funny bone,” which causes a shock-like feeling when bumped because the nerve is so close to the skin.
The ulnar nerve continues down the arm, traveling under muscles within the forearm and into the hand toward the side of the palm with the little finger. As the nerve enters the hand, it travels through another tunnel called the Guyon’s canal.
About
Ulnar neuritis or ulnar nerve entrapment occurs when the ulnar nerve in the arm becomes compressed or irritated. The nerve can be compressed in several places such as the collarbone or wrist; but the most common compression location is the elbow. Depending on the severity of the compression, muscle wasting, a condition where the muscles begin to waste away, can occur. Muscle wasting is particularly problematic because once the muscle is lost, it cannot be rebuilt.
While the exact cause of ulnar neuritis is unknown, there are several factors that can cause pressure on the ulnar nerve:
- The ulnar nerve constantly sliding back and forth from the medial epicondyle can irritate the nerve
- Applying pressure to the elbow for long periods of time
- Fluid buildup in the elbow causing swelling
- A direct blow to the inside of the elbow can cause pain, electric shock sensation, and numbness in the little and ring fingers. This is commonly called “hitting your funny bone
- Prior fracture or dislocations of the elbow
- Bone spurs/ arthritis of the elbow
- Swelling of the elbow joint
- Cysts near the elbow joint
- Repetitive or prolonged activities where the elbow to be bent or flexed
Symptoms
Most symptoms associated with ulnar neuritis occur in the hand.
Symptoms include:
- Intermittent or constant numbness and tingling in the ring finger and little finger, occurring most when the elbow bends.
- Difficulty with finger coordination and weakening of the grip. These symptoms are usually found in more severe cases.
- If the nerve is compressed for a long time or is very compressed, muscle wasting in the hand can occur. Once muscle wasting has occurred, the effects cannot be reversed.
Contact your Florida Orthopaedic Institute physician if any of the listed symptoms are severe but have been present for more than 6 weeks.

Diagnosis
Your Florida Orthopaedic Institute Physician will take a look at your symptoms and examine your arm and hand to determine which nerve is compression and where that nerve is compressed. Your physician may also:
- Check if the ulnar nerve slides out of normal position when elbow is bent.
- Check if the nerve is irritated by tapping over the nerve at the funny bone. If irritated, a shock is felt in the little and ring fingers.
- Check movement in neck, shoulder, elbow, and wrist to see if different positions instigate symptoms.
Treatment
There are many surgical and nonsurgical treatment options available. Nonsurgical options are recommended first, as long as the ulnar neuritis has caused very little to no muscle wasting. If the muscle wasting is severe or if nonsurgical treatments have not helped, surgery may be necessary.
Nonsurgical treatments
Your Florida Orthopaedic Institute physician will recommend nonsurgical treatments unless your nerve compression has caused a lot of muscle wasting. Nonsurgical treatments include:
- Avoid activities where the elbow to be bent for extended periods of time. Keep the elbow straight and do not apply pressure to it.
- If your symptoms just started, your physician may recommend non-steroidal anti-inflammatory medications, such as Advil and Motrin (ibuprofen) or Aleve (naproxen sodium), to help reduce swelling around the nerve.
- Your physician may prescribe a padded brace or splint to wear at night to keep your elbow in a straight position.
- Nerve gliding exercises may also be recommended. These exercises help the ulnar nerve slide through the cubital tunnel at the elbow and the Guyon’s canal at the wrist which can improve symptoms and also help prevent stiffness in the arm and wrist.
Surgical treatments
Your Florida Orthopaedic Institute physician may recommend a surgical treatment to take pressure off of the ulnar nerve pain if nonsurgical methods have not improved your condition, the ulnar nerve is very compressed, or if nerve compression has caused muscle weakness or damage. The surgical treatments currently available include:
- Cubital tunnel release – During this procedure, the ligament “roof” of the cubital tunnel is cut and divided, increasing the size of the tunnel while decreasing pressure on the nerve. As the ligament heals, new tissue grows across the division, expanding the sides of the tunnel. This procedure works best when the nerve does not slide out from behind the bony ridge of the medial epicondyle when the elbow is bent.
- Ulnar nerve anterior transportation – This procedure, unlike cubital tunnel release, will correct the nerve’s location if it has slid out from behind the bony ridge of the medial epicondyle. During this procedure, the nerve is moved to lie either under the skin and fat but on top of the muscle (subcutaneous transposition), under the muscle (sub-muscular transportation), or within the muscle (intermuscular transportation).
- Medial epicondylectomy – In this procedure, part of the medial epicondyle is removed, releasing the nerve. This technique prevents the nerve from getting caught on the boney ridge of the medial epicondyle and stretching when your elbow is bent.
Read the twelve questions you should ask your doctor about ulnar neuritis.
Videos
Related specialties
- Basal Joint Surgery
- Carpal Tunnel Syndrome
- De Quervain's Tenosynovitis
- Dislocated Finger
- Distal Radius Fracture (Broken Wrist)
- Dupuytren’s Disease
- Flexor Tendonitis
- Fractured Fingers
- Functional Nerve Transfers of the Hand
- Ganglion Cysts
- Hand & Finger Replantation
- Hand Nerve Decompression
- Hand Skin Grafts
- Nerve Pain
- Peripheral Nerve Surgery (Hand) Revision
- Revascularization of the Hand
- Rheumatoid Arthritis of the Hand
- Sports Wrist & Hand Injuries
- Sprained Wrist
- Sudden Acute Finger, Hand & Wrist Injuries
- Targeted Muscle Reinnervation (TMR)
- Tendon Transfers of the Hand
- Thumb Ulnar Collateral Ligament Injuries
- Trigger Finger
- WALANT (Wide Awake Local Anesthesia No Tourniquet)
- Wrist Arthroscopy
- Wrist Fractures
- Wrist Tendonitis